












































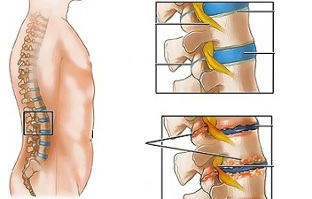
Lumbar osteochondrosis is a chronic disease that develops as a result of a degenerative-dystrophic process in the intervertebral discs. The disease is widespread and affects most people between the ages of 25 and 40.
According to statistics, every second adult experiences back pain at least once in his life, and in 95% of cases it is caused by osteochondrosis of the spine.
Patients with acute lumbar osteochondrosis with persistent pain and other manifestations are considered temporarily disabled. If the situation does not improve within four months, it is decided to establish a disability group.
Lumbar osteochondrosis is a serious medical and social problem because the disease mainly affects people of working age and can lead to the formation of a herniated disc if left untreated.
Causes and risk factors
Factors contributing to the development of lumbar osteochondrosis are:
- anomalies of the spinal structure;
- lumbarization - a congenital pathology of the spine, characterized by the separation of the first vertebra from the sacrum and the transformation of the sixth (additional) lumbar;
- sacralization is a congenital pathology in which the fifth vertebra is connected to the sacrum;
- asymmetrical arrangement of joint spaces of intervertebral joints;
- pathological narrowing of the spinal canal;
- reflected spondyogenic pain (somatic and muscular);
- obesity;
- sedentary lifestyle;
- prolonged exposure to vibration;
- systematic physical stress;
- to smoke.
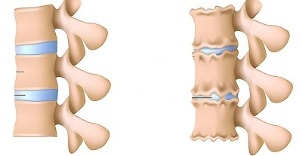
Unfavorable static-dynamic loads, combined with one or more risk factors, cause changes in the physiological properties of the nuclear pulp of the fibrous disc, which play a shock-absorbing role and provide mobility of the spinal column. This process is based on the depolymerization of polysaccharides, which leads to loss of moisture in the tissue of the gelatinous nucleus. As a result, the pulposus nucleus and thus the fibrous disc lose their elastic properties. Additional mechanical stress causes the ring fibrosis to protrude, losing its elasticity. This phenomenon is called protrusion. Cracks form in the fibrous nucleus, causing fragments of the nuclear pulposus to fall out (prolapse, herniated disc).
Prolonged compression of the nerve roots that innervate certain organs of the abdominal cavity over time, worsens their function.
Instability of the spinal segment is accompanied by reactive changes in adjacent vertebral bodies, intervertebral joints, and the accompanying spondyloarthritis develops. For example, a significant muscle contraction in the background of physical activity leads to the displacement of vertebral bodies and the capture of nerve roots with the development of radicular syndrome.
Another cause of pain and neurological symptoms in lumbar osteochondrosis may be osteophytes - processes that cause radicular syndrome or compression myelopathy (compression of the spinal cord) and bone growth in the spinal cord.
Forms of the disease
Depending on which structures are involved in the pathological process, lumbar osteochondrosis is clinically manifested by the following syndromes:
- reflex- lumbosacral, lumboishalgia, lumbago; reflex muscles of the back develop against the background of overstrain;
- compression (spinal, vascular, radical)- compression of the spinal cord, blood vessels or nerve roots causes their development. Examples are lumbosacral radiculitis, radiculoischemia.
Symptoms of lumbar osteochondrosis
Symptoms in lumbar osteochondrosis are determined by which structures are involved in the pathological process.
Lumbago occurs under the influence of hypothermia or physical stress, and sometimes for no apparent reason. The pain comes on suddenly and is of a shooting nature. Intensifies when sneezing, coughing, turning the body, exercising, sitting, walking. In the above case, the pain is significantly weakened. Sensitivity and reflexes are preserved, the rate of movement in the lumbar region is reduced.
Observe on palpation:
- pain in the lower back;
- spasm of paravertebral muscles;
- Straightening of the lumbar lordosis, often associated with scoliosis.
In Lumbago, nerve root tension syndrome is negative. When lifting a straight leg, patients report increased pain in the lower back, not the appearance of an enlarged lower extremity.
Often, lumbar osteochondrosis is a recurrence of more intense and protracted pain attacks.
The clinical picture in lumbodynia is similar to that of lumbosacral pain, but the increase in pain intensity occurs within a few days.
In lumboishalgia, patients complain of pain in one or both lower extremities in the lower back. The pain spreads to the thighs and back of the thighs and never reaches the legs.
Lumboishalgia is characterized by vasomotor disorders:
- changes in skin temperature and color of the lower extremities;
- to feel hot or cold;
- circulatory disorders.
The development of low back pain syndromes is clinically manifested by the following symptoms:
- dermatomal hypalgia;
- shooting pains;
- weakening or complete loss of deep reflexes;
- peripheral paresis.
Pain with compression syndromes increases through twitching, sneezing, and coughing.
Diagnostics
Diagnosis of lumbar osteochondrosis is based on the clinical manifestations of the disease, laboratory and instrumental research methods.
In blood tests against the background of lumbar osteochondrosis:
- decrease in calcium concentration;
- increasing ESR;
- Increased alkaline phosphatase levels.
In the diagnosis of lumbar osteochondrosis, great importance is attached to X-ray examination of the spine.
Prolonged compression of the nerve roots that innervate certain organs of the abdominal cavity over time, worsens their function.
The X-ray signs that confirm the diagnosis are:
- change the configuration of the affected segment;
- pseudospondylolisthesis (displacement of adjacent vertebral bodies);
- deformation of fastening plates;
- intervertebral disc repair;
- Uneven height of the intervertebral disc (sign of gap), which is associated with asymmetric muscle tone.
Used in the diagnosis of lumbar osteochondrosis, if indicated:
- myelography, computed tomography or magnetic resonance imaging - necessary for the development of persistent symptoms, neurological deficits;
- scintigraphy (study of the accumulation of phosphorus by the technologically labeled bone system) - a tumor or an infectious process, performed if there is a suspicion of spinal cord injury.
Differential diagnosis of lumbar osteochondrosis is made with the following diseases:
- spondylolisthesis;
- dyshormonal spondylopathy;
- ankylosing spondylitis (ankylosing spondylitis);
- infectious processes (disc inflammation, spinal osteomyelitis);
- neoplastic processes (primary tumor of the spine or its metastatic lesions);
- rheumatoid arthritis;
- deformed osteoarthritis of the hip joint;
- reflected pain (diseases of the internal organs and large vessels).
Treatment of lumbar osteochondrosis
The following treatment tactics are generally used for lumbar osteochondrosis:
- 2-3 days of bed rest;
- removal of the affected part of the spine;
- strengthen the back and abdominal muscles (create a so-called muscle corset);
- Effect on pathological myofascial and myotonic processes.
Lumbago occurs under the influence of hypothermia or physical stress, and sometimes for no apparent reason.
In most cases, conservative treatment of osteochondrosis of the spine is carried out, including the following measures:
- muscle infiltration anesthesia with local anesthetic solution;
- to take non-steroidal anti-inflammatory drugs;
- intake of sensitizers;
- vitamin therapy;
- to take tranquilizers and antidepressants;
- manual therapy, massage;
- physiotherapy exercises;
- acupuncture;
- isometric relaxation.
Absolute indications for surgical treatment of lumbar osteochondrosis:
- acute or subacute spinal cord compression;
- Development of cauda equina syndrome, characterized by functional disorders of the pelvic organs, sensory and motor disorders.
Therapeutic exercises for lumbar osteochondrosis
Physical therapy plays an important role in the complex treatment of osteochondrosis of the spine. Regular exercise allows you to normalize the muscle tone of the paravertebral muscles, improve metabolic processes in the tissues affected by the pathological process, and in addition create a well-developed muscle corset that can keep the spine in proper position and remove unnecessary static loads.
For gymnastics with lumbar osteochondrosis to have the greatest effect, you must follow the following principles:
- regularity of lessons;
- gradual increase in the intensity of physical activity;
- Avoid overwork during class.
Physiotherapy should be performed under the guidance of an experienced trainer who will select the exercises that are most effective for a particular patient and monitor the correctness of their implementation.
According to statistics, every second adult suffers from back pain at least once in his life, in 95% of cases it is caused by osteochondrosis of the spine.
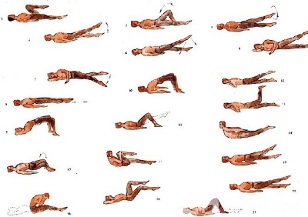
In addition to classes with an instructor, you should do a series of morning exercises on a daily basis, including specific exercises for lumbar osteochondrosis.
- Relaxation and contraction of abdominal muscles.The starting position is on the feet, feet shoulder-width apart, lowered to the body at intervals. Breathe smoothly, relaxing the muscles of the anterior abdominal wall. During exhalation, pull the culture in as much as possible by tightening the abdominal muscles. The exercise should be repeated until a slight fatigue appears.
- Head movements with bending of the spine.The starting position is kneeling, with the arms outstretched, the back straight to the ground. Slowly lift your head and bend at the waist. Hold this position for a few seconds and smoothly return to the starting position. Repeat at least 10-12 times.
- "Pendulum".The starting position is stretched on your back, the arms, knees and hips are bent at an angle along your body. In a swinging pendulum-like motion, turn your feet left and right, trying to reach the ground. In this case, the shoulder blades cannot be torn off the ground.
- boat.The starting position is stretched on your abdomen, arms are stretched forward. Bend at the back and pull the upper body and legs off the ground. Hold this position for 5-6 seconds and slowly return to the starting position. Avoid 10 times.
Potential consequences and complications
The main complications of lumbar osteochondrosis are:
- formation of intervertebral hernia;
- vegetative-vascular dystonia;
- spondylolysis, spondylolisthesis;
- osteophytosis;
- spondyloarthritis;
- Narrowing of the spinal canal, which leads to compression of the spinal cord and can lead to permanent disability and reduced quality of life.
Prolonged compression of the nerve roots that innervate certain organs of the abdominal cavity over time, worsens their function. As a result, patients have intestinal dysfunction (constipation, diarrhea, abdominal cavity) and pelvic organs (urinary disorders, erectile dysfunction, cold, infertility).
Forecast
Pain syndrome in lumbar osteochondrosis occurs in the form of remission and exacerbation. Lumbago lasts 10-15 days, after which the patient's condition improves and pain decreases. A favorable outcome can prevent related secondary diseases. Often, with osteochondrosis of the spine there is a recurrence of more intense and prolonged pain attacks.
Physical therapy plays an important role in the complex treatment of osteochondrosis of the spine.
Patients with acute lumbar osteochondrosis, persistent pain and other manifestations are considered temporarily disabled. If the situation does not improve within four months, it is decided to establish a disability group.
Prevention
Prevention of the development of osteochondrosis of the spine consists of the following measures:
- quit smoking;
- normalization of body weight;
- improvement of general physical condition, active lifestyle;
- Avoid provocative conditions (lifting weights, sudden movements, bends, bends).